
The personal fat threshold

From the American Institute for Cancer Research
Before we talk about personal fat threshold's, let's quickly talk about insulin resistance.
WHAT IS Insulin Resistance?
To get an idea of what insulin does, check this out – insulin the basics. With this understanding it is easier to grasp what insulin resistance is and also get closer to understanding about metabolic dysfunction and metabolic flexibility. Insulin has a central role in energy substrate partitioning ie how well we can burn our fat stores, how easily we can switch between burning carbs and fat. Resilience lies in this flexibility. Insulin resistance is complex and the science is always progressing as new information is discovered.
It is important to understand the concept because this idea is tied up as a causative factor in chronic illness that is restricting our ability to live long, medication free, enjoyable lives.
We can be transiently ‘insulin resistant’, which in certain situations is thought to be beneficial to us – for example in critical illness. This ‘physiological’ insulin resistance which can also be noted in some on a very low carb diet, is thought to exist to free up glucose for use by tissues that can’t use any other energy substrate e.g ketones or fatty acids. We could call this ‘glucose sparing’ to prevent confusion. Is prolonged physiological insulin resistance good for us? – that’s a great question that there are no definitive answers to, yet.
When a person is chronically ‘insulin resistant’, insulin persistently doesn’t have the designed effect on the tissues it is destined to impact. The insulin doesn’t work effectively to allow energy into the cell. Also, as insulin levels build and build to force a change, these high levels don’t allow you to burn the fat in the cell. We are stuck.
For example, an insulin resistant fat cell is the end result of too much energy (glucose/fatty acids) than our system needs. Extra glucose, extra fat that our bodies don’t require for the amount of work it’s doing. A fat cell (adipocyte) that is too full, already stuffed, bulging with stored energy becomes resistant to insulin, basically saying “I can’t take any more energy, there’s no room!!“. So it refuses insulin’s actions. The insulin whose job here is to knock on the door and get the fat into the cell, fails at its task = insulin resistance.
Agitated and angry, despite one of insulin’s jobs being keeping energy inside cells, the fat cell spews out some of its fat into the blood stream – the triglycerides it stores.
This inflamed, angry fat tissue causes all sorts of immune responses, cytokines cascade and white cells march to the area, but the cause of the inflammation cannot be fixed by these responses, the inflammation becomes chronic, resulting in the pro – inflammatory environment associated with many chronic diseases.
This occurs at our ‘personal fat threshold’. A threshold that’s differs between people and ethnicities. Once we meet that threshold, the pathological effects of having too much energy flowing through our blood begin. This can happen at any weight.
The pancreas in an effort to try and shove the fat back into the fat cell, makes more insulin, this high baseline of insulin is hyperinsulinaemia. This maybe where the affects of physiological insulin resistance and pathological (disease causing) insulin resistance seperate themselves.
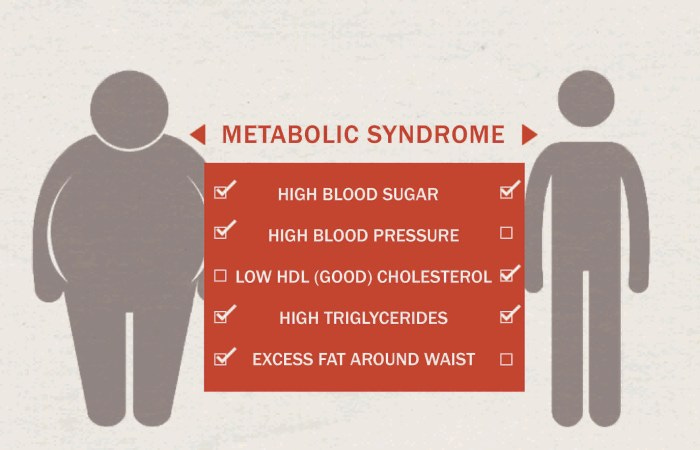
When we run out of room in our fat cells we start to store fat in places there should be no fat – around the organs in our abdomen (this is why waist circumference is a helpful tool), in our organs – Non alcoholic Fatty liver disease, around our heart, not good.
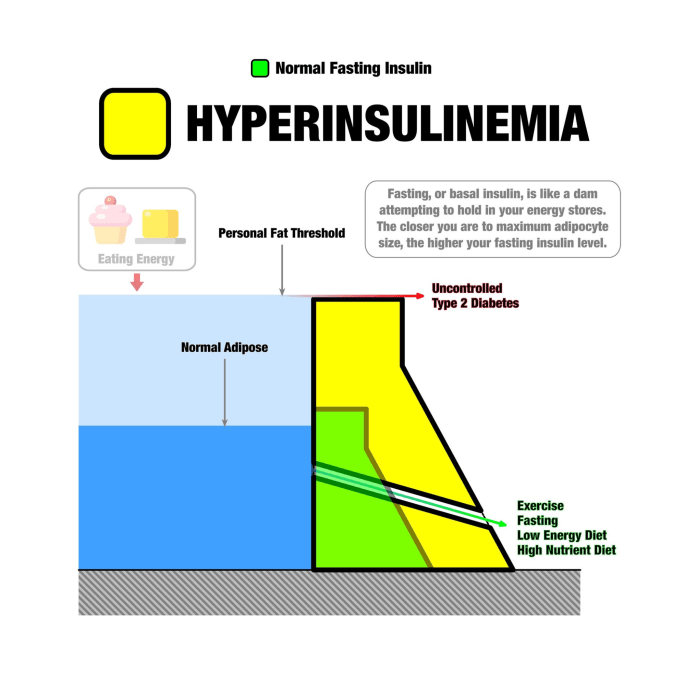
Infographic courtesy of Ted Naiman (www.burnfatnotsugar.com)
Even if we haven’t eaten anything recently, if there is more glucose and fat in our diet than our body needs, the effort of keeping the fat in the cells requires a high base line of insulin. This is easy to do with frequent consumption of ultra-processed foods that are high in both refined carbohydrate and refined fat AT THE SAME TIME.
Eventually this situation can result in disease states such as type 2 Diabetes. In type 2 diabetes we’ve reached our personal fat threshold, the insulin we make is it isn’t very effective anymore, the fat tissues just don’t respond to it and we make more and more insulin to try an counteract this. So now in our blood stream we’ve got excess sugar that can’t get into the cells and excess fat thats leaking out of them, causing inflammation AND lots of insulin – bad news. Energy substrates aren’t meant to be hanging around in our blood stream.
Insulin resistance and hyperinsulinemia are now understood to be a baseline, important mechanistic causes of many chronic diseases and health issues – type 2 diabetes, dementia, cancer, heart disease, strokes, erectile dysfunction, mood disorders, gut disorders, the list goes on.
Different cells can have different amounts of insulin resistance. Your muscles can be more or less insulin resistant than your liver or your kidney – all can have different results in tests that we do, but all are caused but the same thing resulting in different problems.
Your insulin resistance is directly related to the SIZE of your adipocytes (fat cells). The fatter and more chock full your adipocytes are – the more insulin resistant you will get.
A subset of people can make more fat cells. Little tiny fat cells ready to accept all the excess energy that we don’t use. These people can become incredibly overweight without evidence of metabolic dysfunction, that is without the excess triglycerides and glucose stuck in the blood stream, without the ectopic fat stores around the organs or in the liver. These people are NOT most people.
Those of us that don’t make more fat cells try and jam the fat in the cells we already have and exhibit the signs of metabolic dysfunction or metabolic syndrome. 1 in 4 of the adult UK population is thought to qualify as having metabolic syndrome resulting in significantly increased risks of things we are scared of – cancer, heart disease, stroke, and numerous other illnesses that we seem less scared of but that are just as significant and life shortening.

The Personal Fat Threshold is different for us all. Signs of metabolic syndrome means we are at it!
The fast road to reaching your personal fat threshold is eating a combination of ultra-processed carbs and processed fat (refined vegetable oils).
These types of hyperpalatable foods are designed to make it hard to stop eating. They activate dopamine receptors making us feel good, they cause swings in blood sugars resulting in lots of hunger and they switch off satiety centres so we just don’t feel full. The result is excess energy that we don’t need and have to find storage for, with very little nutrient density.
‘Keeping intake to levels that support exercise but not body fat’ as Crossfit HQ supports is incredibly difficult on a highly processed diet that’s full of both ultra-refined carbs and refined fats, it has very little to do with will power. If we want to stave off chronic illness and keep active until our 90’s, these ideas are central to our success.
How to combat this?
Eat protein led, nutrient dense whole foods.
Build bigger muscles - muscles are the biggest sink for glucose and fat to be stored and then quickly used.
For some insight into my thoughts on optimum nutrition check this.
Optimum nutrition, a framework for decision making
Alberti KG, Zimmet P, Shaw J; IDF
Epidemiology Task Force Consensus Group. The metabolic syndrome a new worldwide definition. Lancet
2005;366:1059-62
